
What is happening in this electrogram?
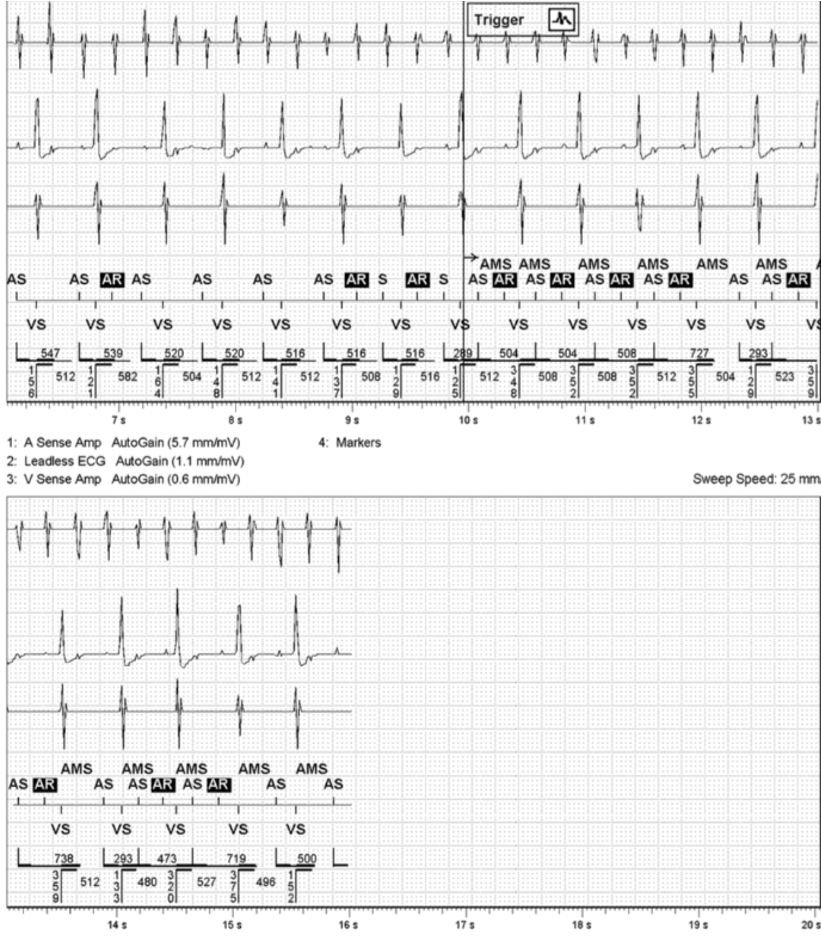
This EGM was stored as an AMS episode. Flutter waves are visible on the atrial sense amp channel but notice the marker channels are not marking every wave. This means that the waves are falling into blanking (PVAB: post ventricular atrial blanking). In this device, the nominal setting for PVAB is 150ms.
Is this appropriate device behavior?
Answer:
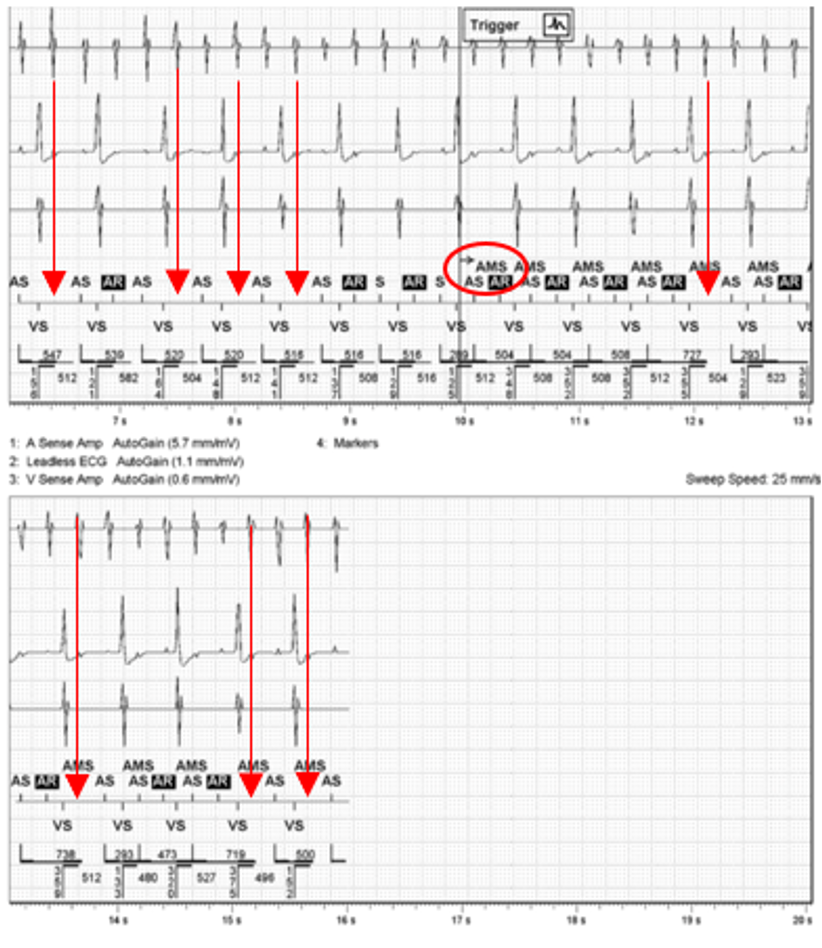
This is an appropriate mode switch; however, the device should have mode switched sooner and would have if the waves were not falling into the blanking period. It is important to consider the implications of the blanked waves.
- We can clearly see the flutter waves, but since the device is not seeing them, how long has this patient been in flutter?
- What is the true AF burden?
It is evident that after the device mode switches, some waves continue to fall into the blanking period and are not being counted. This behavior can cause the device to enter and exit a mode switch even when there is a true atrial arrythmia occurring. While this may not cause concern for a patient who is already anticoagulated, it could pose a problem for someone with no prior history of AT/AF. It is important to point out that in this case, the patient is not pacemaker dependent. Consider a patient with complete heart block. A patient with CHB would track the waves that the device is seeing, oftentimes at the max track rate before finally mode switching. This may cause the patient to become symptomatic.
What, if any, programming changes would you recommend?
Answer:
In this situation, decreasing the post ventricular blanking period would be an appropriate programing change.
It is best to use calipers to measure the V-to-A interval for the AF waves that are falling into the blanking period. If for example, the wave was being blanked at 120ms, it would be appropriate to program PVAB from 150ms to 110ms. PVAB can be programmed from 60-250ms in this device. Reprogramming PVAB should be evaluated carefully. Programming PVAB too short can cause far field R wave oversensing and inappropriate mode switches, while programming PVAB too long can potentially mask arrhythmias. This is especially important in ICDs and SVT discrimination, i.e. V>A.


