
By Kimberly O’Donogue
This dual chamber ICD (Abbott) patient presented to a routine device clinic check in Spring 2022. This patient declined remote monitoring, so we were checking them every three months. There was a note in the device that stated there is a history of Non-Sustained RV Oversensing and at this time it was being monitored and technical services were aware as was the physician. I interrogated the device, but noticed the NSRVO recordings looked a little different than before.
Threshold/Sensing/Impedance measurements were all stable.
Figure 1 and Figure 2:
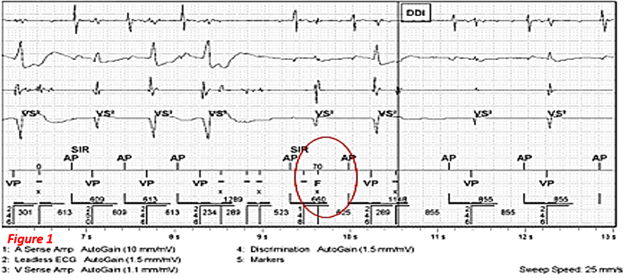
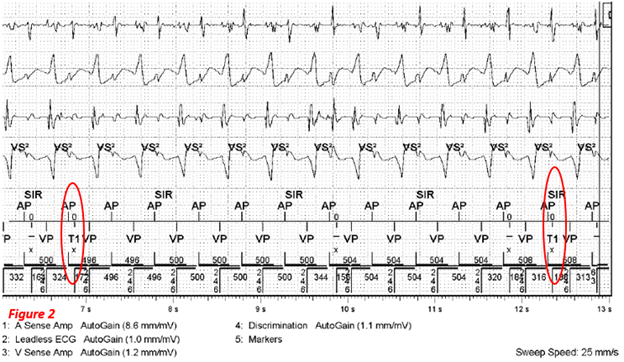
Why was this different? As you can see, the device started to bin some of the intervals into the therapy zones. I called Tech Services and was advised that this lead needed to be revised. I discussed the findings with the physician, and we turned therapies off. The patient was sent for a consultation. (The patient has this device for primary prevention and never has had therapy)
The patient presents to device clinic three months later….
To my surprise, the lead was not revised, and therapies were still off. The patient informed me that she was too nervous to go through an extraction and wanted to wait until it was time for her to get a generator change (estimated remaining life was 1.2 years), and she would decide what to do with that wire at that time. I completed a full device interrogation.
- Device measurements remain stable.
- Programmed DDDR 70/130 w VIP- Tachy Disabled
- No AMS/VT/VF
- Pt is AP >99% and VP <1%
- Underlying Rhythm is Sinus Brady appx 50bpm- PR interval appx 168ms
I was just about to wrap things up when I noticed this on my programmer screen: (Figure 3)
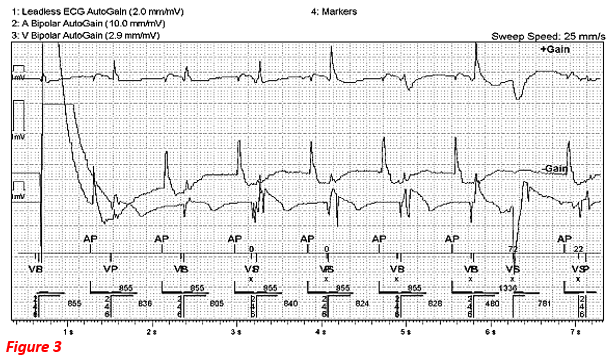
The marker channels are hard to see, but the device is ventricular safety pacing (VSP). Why does a device VSP? Crosstalk! How does the device decide if crosstalk is present? If the ventricular-sensing amplifier senses any event during the crosstalk sensing window, VSP is delivered, usually 100-110ms after the atrial event.
Is this cross talk?
Is this appropriate device behavior?
Do we need to reprogram anything?
Answer:
This is NOT crosstalk.
Remember, this patient has a history of RV lead noise. It appears the device thinks it is seeing crosstalk.
Why was I concerned about this?
- Pace on T! The patient has a defibrillator though, right? Remember, it’s currently OFF due to noise and the potential for inappropriate therapies. Let’s say if this did happen, this patient would potentially be in big trouble.
What did I do?
- I discussed my concerns with the following physician, and we reprogrammed the patient from DDDR to AAIR.
Why did I share this?
- This was certainly NOT a normal device check for many reasons. It would be easy to breeze through it knowing there is noise, and simply move on. The device is off, right? While this is certainly a one off, our job as techs is to fully check the device and provide the physician with the best possible information. Am I paranoid? Maybe. However, patient safety is #1. If the physician didn’t want it reprogrammed, that would have been okay too. I knew I did what I felt was best for the patient and that’s all I can do.


